Chronic scarring
Diabetes, high blood pressure, inherited disease, and long-running inflammation can gradually reduce kidney function.
Patient guide + clinician detail
Kidney failure is not one single disease. It is the end result of different problems that damage the blood filters, reduce blood flow, block urine drainage, inflame the kidney, scar it slowly, or overwhelm it suddenly.
First principle
Think of the kidneys as blood-cleaning organs. They remove waste into urine, balance water and salts, help control blood pressure, help make red blood cells, and support bone chemistry. Kidney failure means those jobs are no longer being done well enough.
The tricky part is that kidney disease can be quiet for years. Some people feel normal until blood tests, urine tests, swelling, high blood pressure, or a sudden illness reveals the problem.
Frame the presentation by tempo, substrate, and syndrome: AKI, AKD, CKD progression, ESKD, or AKI-on-CKD. Etiology is often inferred from trajectory, urine sediment, albuminuria/proteinuria pattern, imaging, medication exposures, hemodynamics, systemic features, and prior eGFR/UACR data.
Stabilization and etiology workup run together: potassium, acid-base status, volume status, uremic complications, obstruction, nephrotoxins, glomerular emergencies, sepsis, rhabdomyolysis, TMA, paraprotein disease, and dialysis indications.
Patterns
Diabetes, high blood pressure, inherited disease, and long-running inflammation can gradually reduce kidney function.
Dehydration, shock, sepsis, medicines, contrast, toxins, rhabdomyolysis, or severe inflammation can cause a sudden drop.
Prostate enlargement, stones, tumors, strictures, clots, or catheter problems can make urine back up into the kidneys.
Infection, low blood pressure, heart failure, dehydration, NSAIDs, ACEi/ARB changes, obstruction, or contrast may destabilize CKD.
Cause map
Diabetes is one of the most common causes of kidney failure. Over time, high blood sugar can injure the tiny filters in the kidneys. High blood pressure often travels with diabetes and adds more strain.
Clue: early diabetic kidney disease may show up as albumin protein leaking into the urine before symptoms are obvious.
Diabetic kidney disease usually presents with persistent albuminuria and/or declining eGFR in the context of diabetes, often with hypertension and cardiovascular disease. Keep the differential open when the course is atypical: active sediment, abrupt nephrotic syndrome, rapid eGFR loss, short diabetes duration, absent retinopathy in type 1 diabetes, or systemic features.
High blood pressure can narrow and damage kidney blood vessels. Damaged kidneys can then make blood pressure harder to control, creating a cycle that may end in kidney failure.
Why it matters: blood pressure control is one of the biggest kidney-protection steps for many people.
Hypertensive nephrosclerosis is a clinical diagnosis, but evaluate for renovascular disease, primary aldosteronism, sleep apnea, medication contributors, APOL1-associated disease where relevant, malignant hypertension, and thrombotic microangiopathy when severity or trajectory does not fit routine essential hypertension.
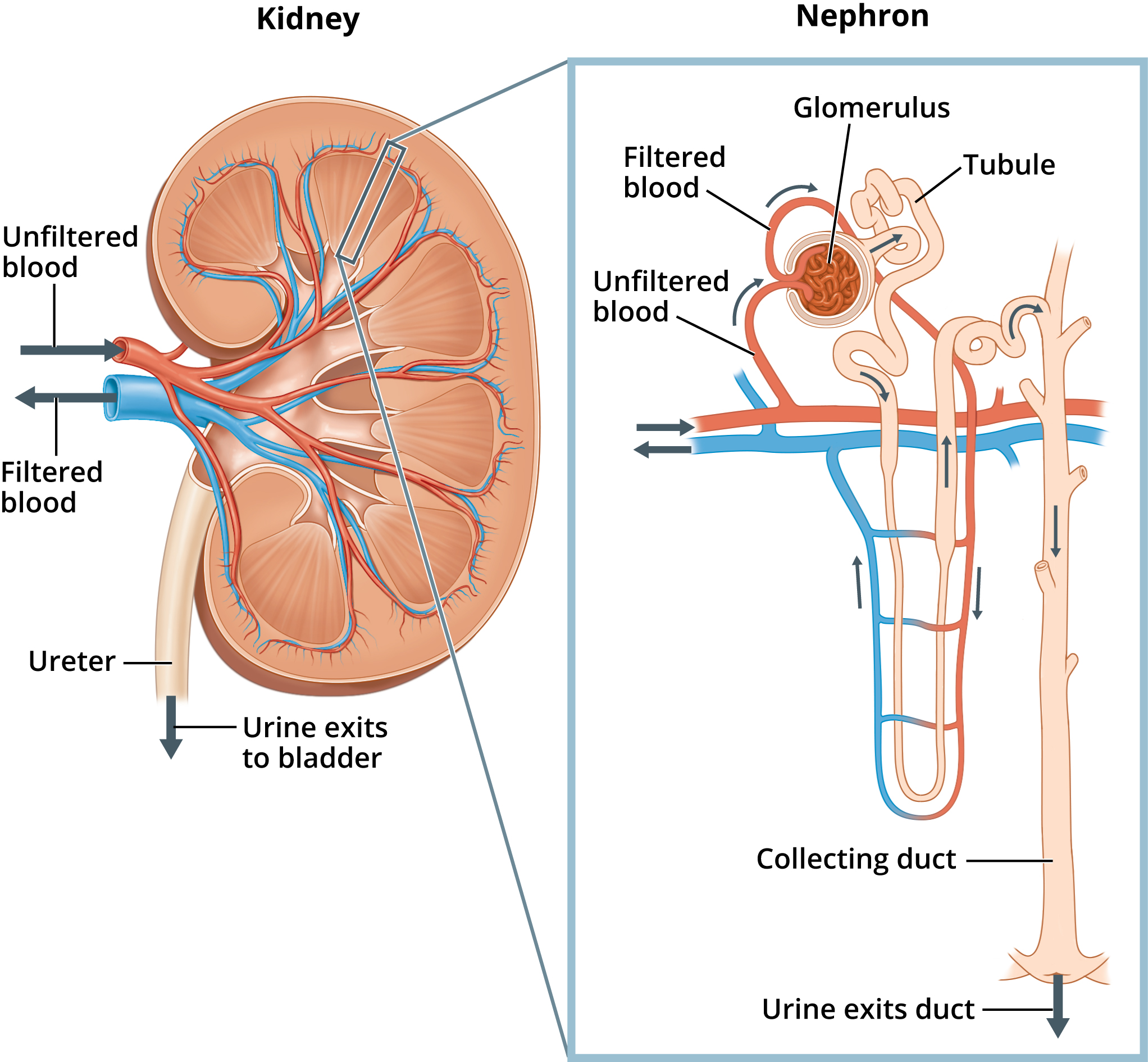
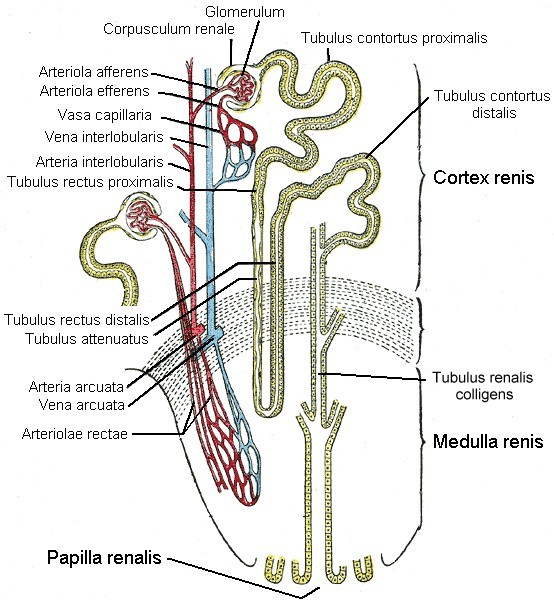
The glomeruli are tiny blood filters. Immune problems can inflame them, causing blood or protein in the urine, swelling, high blood pressure, and sometimes fast kidney failure. Examples include IgA nephropathy, lupus nephritis, vasculitis, and nephrotic syndromes.
Clue: cola-colored urine, foamy urine, or swelling around the eyes and legs deserves medical evaluation.
Active sediment, dysmorphic RBCs, RBC casts, heavy proteinuria, low complement, systemic symptoms, pulmonary hemorrhage, rash, neuropathy, or rapidly progressive eGFR decline should trigger glomerulonephritis evaluation. Consider IgAN, lupus nephritis, ANCA vasculitis, anti-GBM disease, membranous nephropathy, FSGS, infection-related GN, C3G, and monoclonal gammopathy-related disease.
Kidneys need steady blood flow. Dehydration, major bleeding, sepsis, severe vomiting or diarrhea, heart failure, liver failure, or very low blood pressure can suddenly reduce filtration.
Good news: some blood-flow kidney injuries improve when the cause is treated early, but prolonged injury can damage the tubules.
Prerenal physiology can progress to ischemic ATN when hypoperfusion is severe or sustained. Assess effective arterial blood volume, venous congestion, cardiac output, sepsis physiology, hepatorenal syndrome phenotype, urine microscopy, FeNa/FeUrea limitations, nephrotoxin exposure, and response to carefully chosen volume or decongestion strategy.
Some medicines can stress the kidneys, especially during dehydration or illness. NSAID pain relievers such as ibuprofen and naproxen, some antibiotics, chemotherapy, immune medicines, contrast dye, lithium, and certain supplements or toxins may contribute.
Important: never stop a prescribed medicine without medical advice, but do tell clinicians every medicine and supplement you use.
Consider hemodynamic AKI from NSAIDs/RAAS blockade/diuretics, ATN from aminoglycosides or cisplatin, AIN from beta-lactams/PPIs/NSAIDs/checkpoint inhibitors, crystal nephropathy, pigment nephropathy, oxalate nephropathy, contrast-associated AKI, lithium-related CKD, calcineurin toxicity, and herbal/heavy-metal exposures.
If urine cannot drain, pressure can build backward into one or both kidneys. Causes include prostate enlargement, stones, tumors, strictures, blood clots, pelvic masses, or a blocked catheter.
Clue: trouble urinating, lower belly pain, flank pain, recurrent infections, or suddenly reduced urine output may point to obstruction.
Postrenal AKI is treatable and easy to miss. Check bladder volume/catheter patency, renal ultrasound for hydronephrosis, medication-related retention, prostate disease, stones, malignancy, retroperitoneal fibrosis, neurogenic bladder, ureteral injury, and bilateral or solitary-kidney obstruction.
Some kidney diseases run in families or begin with a structural problem. Polycystic kidney disease can cause many cysts to grow in the kidneys. Reflux, congenital urinary tract problems, Alport syndrome, and other inherited conditions can also lead to kidney failure.
Clue: family history, early high blood pressure, hearing problems, cysts, or kidney disease at a young age may matter.
Include ADPKD/ARPKD, Alport spectrum, congenital anomalies of the kidney and urinary tract, reflux nephropathy, medullary cystic/tubulointerstitial kidney diseases, complement-mediated disorders, and APOL1-associated nephropathy. Family history may be absent because of de novo variants, small families, adoption, or underdiagnosis.
Kidneys can be injured by severe infections, repeated kidney infections, kidney stones, autoimmune disease, blood cancers such as myeloma, muscle breakdown, pregnancy complications, and illnesses that affect small blood vessels.
Pattern: kidney failure sometimes reflects a whole-body problem, not a kidney-only problem.
Keep pyelonephritis with obstruction, sepsis-associated AKI, TMA, myeloma cast nephropathy, tumor lysis, rhabdomyolysis, sickle nephropathy, sarcoidosis, oxalosis, urate nephropathy, pregnancy-associated preeclampsia/HELLP/TMA, and infiltrative malignancy on the list when the presentation is systemic or the data do not fit common CKD.
Safety
Kidney failure can become dangerous because fluid, acid, and potassium can build up in the blood. Severe infection, blocked urine, and sudden kidney injury need quick attention.
The patient-facing symptoms below map to oliguria/anuria, pulmonary edema, hyperkalemia, uremic encephalopathy, obstructed infected system, severe AKI, and hypertensive emergency. Clinical priorities are potassium, ECG, acid-base status, volume status, obstruction search, nephrotoxin hold, infection control, and dialysis threshold.
Workup
Creatinine and eGFR estimate how well the kidneys filter. Electrolytes, especially potassium and bicarbonate, show whether failure is becoming dangerous.
Urinalysis and urine albumin-to-creatinine ratio can show blood, protein, infection, crystals, or inflammation that points toward a cause.
Ultrasound can look for blocked urine flow, kidney size, cysts, swelling, or clues that disease is longstanding.
Doctors may check diabetes, blood pressure, immune markers, infection tests, medicine exposures, inherited disease, or sometimes do a kidney biopsy.
BMP/CMP with potassium and bicarbonate, creatinine trajectory, BUN, calcium/phosphate, magnesium, CBC, venous or arterial blood gas when indicated, uric acid/CK/LDH by context, ECG for hyperkalemia risk, strict I/O, weight, and volume assessment.
Urinalysis with microscopy, UACR/UPCR, urine culture when indicated, sediment review for casts/crystals/dysmorphic RBCs, and cautious interpretation of urine electrolytes in diuretic use, CKD, contrast exposure, and mixed physiology.
Renal/bladder ultrasound for hydronephrosis, bladder retention, kidney size/echogenicity, cystic disease, and solitary kidney. Use CT/MRI, Doppler, or vascular imaging when stones, malignancy, renal vein thrombosis, infarction, or renovascular disease remain plausible.
HbA1c, complement, ANA/dsDNA, ANCA, anti-GBM, hepatitis/HIV, SPEP/UPEP/free light chains, PLA2R, pregnancy testing, tox/medication review, and biopsy when results will change treatment and bleeding risk is acceptable.
Medical visuals
Sources